HARDWARE SUTURE IN LAPAROSCOPIC AND MINIMALLY INVASIVE SURGERY
Mechanical staplers have been used in abdominal surgery since the middle of the last century. Most of them were developed by domestic scientists for anastomosis in areas that are hard to reach for manual suture. The advantages of a hardware suture have been identified in open operations:
- minimal trauma (hardware suture has always been distinguished by a softer and less traumatic effect on tissues than the application of the same number of manual sutures);
- minimal invasiveness (the time during which the intestinal lumen remains open is significantly reduced, the potential for contamination of the abdominal cavity is reduced);
- simplification of operational technique (ease of use in hard-to-reach places, simplification of mobilization and anastomosis in case of discrepancy between the diameters of the ends of the intestine, etc.);
In addition, many authors emphasize the high reliability of hardware anastomosis. All of these positive characteristics contribute to obtaining favorable clinical results. Staple staplers are the most widely used. Most of them were developed by simply adapting already existing staplers to laparoscopic surgery for possible insertion through narrow trocar ports, the other part was designed anew.
The principle of a hardware seam is to connect tissues using metal clips (brackets), which, depending on the application, have a different shape. Titanium staples are used in modern foreign models. The latest in hardware suture technology is the use of absorbable staples (“POLYSORB”), which completely dissolve in the body in about 180 days and are widely used for suturing tissues, forming anastomoses, ligating vessels, etc.
The scope of staplers in laparoscopic colorectal surgery can be divided into 2 areas: for anastomosis and for mobilization of the corresponding segments of the colon. Steichen et al. There are the following ways of using staplers:
- lateral and tangential excision of the intestine and linear suture of the intestine;
- resection of the intestine and the imposition of a linear functional end-to-end anastomosis (right-sided hemicolectomy, resection of the transverse colon, etc.);
- resection of the intestine and the imposition of an end-to-end circular anastomosis through the natural openings of the body (anus), for example, during resection of the rectum or sigmoid colon;
- resection of the intestine and the imposition of a circular two-row anastomosis through an additionally performed anterior perineotomy (low and ultra-low anterior resection of the rectum).
CIRCULAR STAPLERS
The use of a circular stapler in rectal surgery can significantly increase the proportion of sphincter-preserving operations. The device allows to carry out low anterior resections of the rectum for those patients who previously underwent abdomino-perineal extirpations and abdomino-anal resections with colostomy removal. For the convenience of passing through the physiological bend of the rectum when performing high anterior resections and resections of the overlying sections of the rectum, since the 80s of the 20th century, devices have been produced with a bend of the working part and with a removable head. The presence of the latter makes it especially convenient for performing laparoscopic operations. The device imposes a two-row staple seam.
In our practice for open resections of the colon, we widely used a reusable steel holder of a circular stapler with replaceable disposable cassettes. The design of this device does not allow removing the head, which makes it less convenient to use.
Significantly reduces the time of the operation by applying a purse-string suture using a hardware technique.
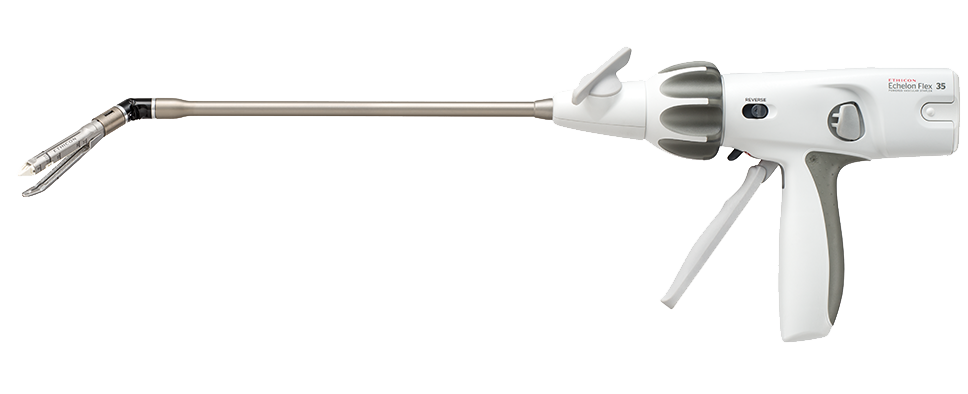
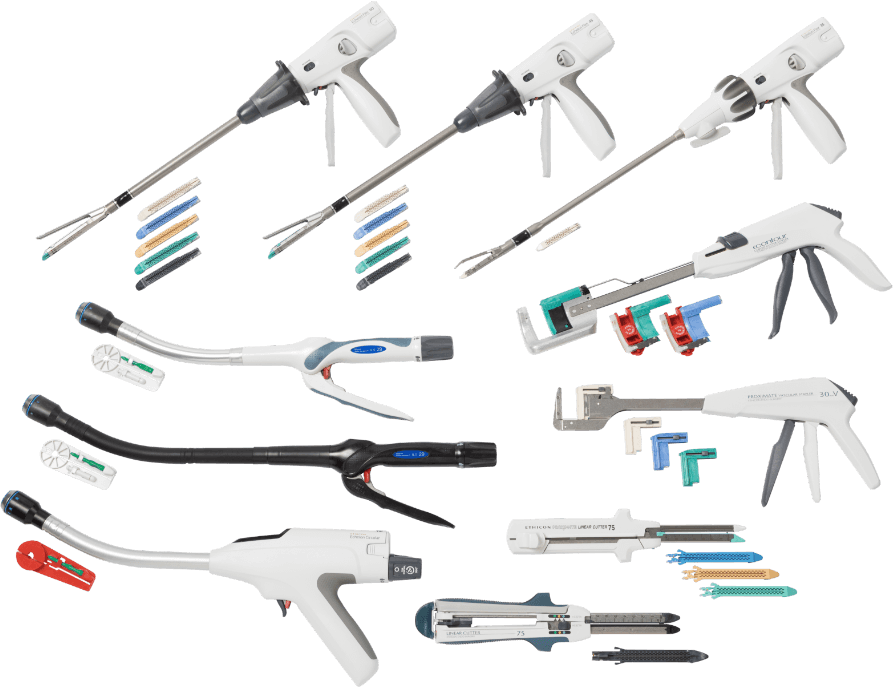
LINEAR STAPLERS
The GIA apparatus is an improved analogue of the domestic NLCA and is mainly used for anastomoses. The GIA places two rows of sutures on each side and crosses the tissue to be sutured between them with a knife. Modern devices have a number of advantages. Firstly, a tissue gap control mechanism has been introduced, which ensures their convergence to a certain distance before stitching. Secondly, not tantalum, but titanium clips are used in the devices.
In 1991, devices ENDO-GIA-30, ENDO-TA-30 were created specifically for endosurgery. Outwardly, they are completely different from their counterparts, but the principle of operation remains the same, only a three-row seam is applied instead of a two-row one. With the advent of these devices, it became possible to perform all stages of resection of the colon and stomach intracorporeally. The scope of these tools is similar to that indicated above.